

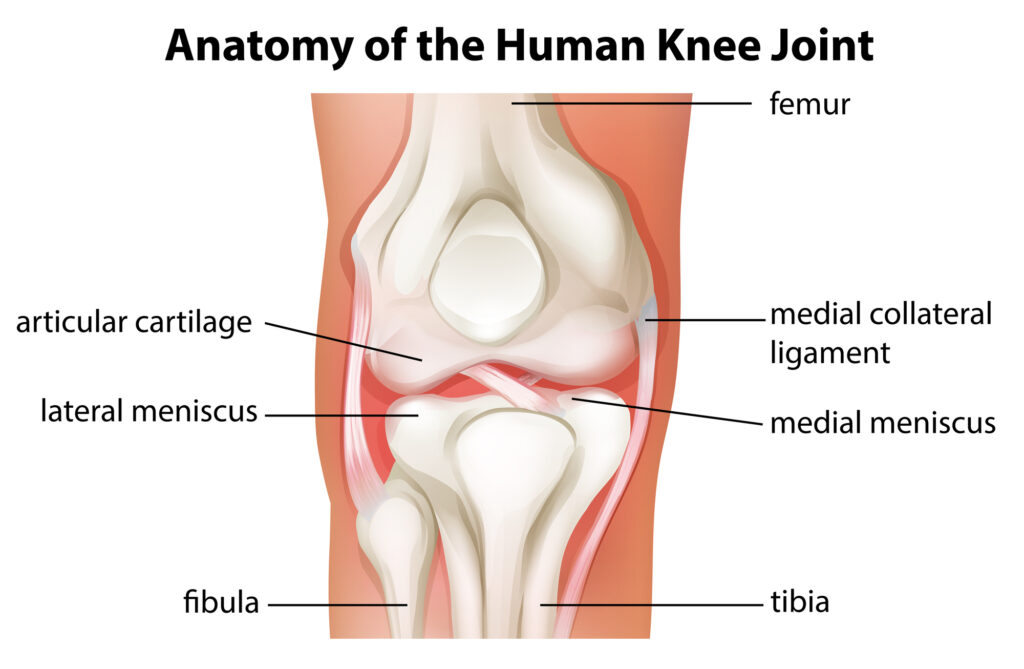
The meniscus is a C-shaped pad of fibrocartilage that sits between the femur and the tibia within the knee. Each knee has a medial (inner) and lateral (outer) meniscus. The function of the meniscus is to act as a cushion for the cartilage surfaces of the knee joint. The meniscus is like a shock absorber that helps to absorb stress and decrease contact pressures on the cartilage. When the meniscus is damaged, it can lead to cartilage wear or damage, and cartilage wear is also known as arthritis.
Meniscal injuries are very common and can occur with a variety of activities, from high energy sporting injuries, to relatively benign twisting or deep flexion injuries to the knee. The meniscus has a relatively poor blood supply, which makes it more vulnerable to injury and prevents it from healing on its own. Especially as we age, the tissue quality of the meniscus weakens and thus it becomes more susceptible to tearing. In a young patient (under 20) it takes a high energy injury usually to cause a meniscal tear. As we age, especially into our 40s, 50s, 60s, the meniscal tissue begins to degenerate and degenerative type tears are common and occur often without significant injury.
Types of Meniscus Tears
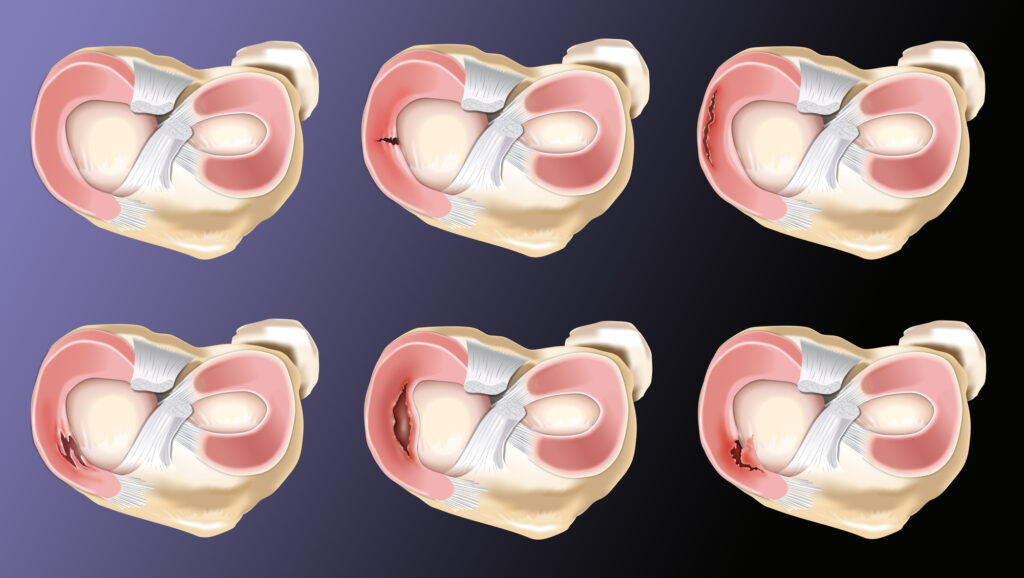
There are several types of meniscal tears, see image below, and these different types of tears cause different symptoms. These symptoms can vary from relatively no symptoms to pain, swelling, and mechanical symptoms such as popping, locking, or catching sensations.
Displaced Meniscal Tears
Displaced meniscal tears (like bucket handle tears or radial flap tears) can cause pain and mechanical sensations in the knee. It can be thought of like a hangnail on your finger. When the hang nail is in normal position it may not hurt, but when you put your hand in your pocket and the hang nail gets pulled back, it causes pain. This is very common for displaced meniscal type tears that may be asymptomatic at times, but other times the tissue may get twisted or pulled and irritate the cartilage surface of the joint, causing pain.
Degenerative Meniscal Tears
Degenerative type meniscal tears, or horizontal cleavage type tears, rarely cause mechanical symptoms and instead present as pain, or sometimes do not cause symptoms at all. Surgery for these types of tears is rarely indicated, and some studies suggest can actually worsen arthritic changes. Sham surgery studies on patient’s with degenerative meniscus tears and arthritis showed that those patients who had a true partial meniscectomy did no better than the patient who had just the incisions made but no actual surgery performed!
How are Meniscus Tears Diagnosed?
Diagnosis of a meniscus tear is completed with a thorough history and physical exam which confirms pain along the joint line and often pain with flexion and twisting of the knee, reproducing symptoms. Xrays are often taken to assess how much arthritic change is present in the knee which can be seen by assessing the space between the bones. The less space present indicates less cartilage covering on the ends of the bones which tells us that it is very likely there is a degenerative type meniscal tear. Usually in these cases however, treatment of the arthritis is indicated, not surgery to address the meniscus. An MRI may be ordered to confirm the diagnosis of meniscal tear and this is usually done when surgery is being planned to help prepare for the surgery.
How are Meniscus Tears Treated
There are many treatment options for meniscal tears, and the majority of these tears we see in the office can be managed without surgery. Just because you have a meniscus tear doesn’t mean you necessarily need surgery! Often we can treat meniscal injuries conservatively and will often begin with ice, rest, NSAIDs, possibly a cortisone injection and a physical therapy program.
The goal of this treatment is to improve symptoms and pain. The meniscal tear will not heal, but if it doesn’t bother you anymore, surgery is not necessary. The goal of physical therapy is to strengthen the hip, gluteal muscles, quadriceps and hamstrings while improving hamstring and iliotibial band flexibility. This all helps to decrease joint reactive forces on the knee, by making the surrounding muscles do the work and see the load, the joint sees less stress and you feel less pain. It really works!
When this doesn’t work, you may be indicated for arthroscopic surgery for either meniscal repair, or partial meniscectomy, removal of the torn piece.

Surgery
In young patients, under 25, we tend to be more aggressive with surgery to try to arthroscopically repair the meniscus tissue if possible to preserve the meniscus. Saving the meniscus tissue theoretically protects the cartilage surfaces of the joint over time, decreasing risk of progression of arthritis. This however must be balanced with the knowledge that not all meniscal tear patterns are repairable, and that at certain ages (over 40) the ability for the body to heal the repair goes down and thus may not be worth the longer recovery.
In older patients, or patient’s with tears that are not repairable or will not heal, we tend to proceed with arthroscopic partial meniscectomy to remove the torn piece, aka trim the hangnail, removing the irritant from the knee. Pain coming from this piece irritating the knee will improve, but this surgery cannot restore or repair worn or damaged cartilage in the joint.
Recovery
Recovery after surgery varies. For partial meniscectomy patients can expect typically a 6-12 week recovery. You are walking and working on knee exercises right away and starting formal physical therapy early is critical for a good functional outcome. For meniscal repairs, the typical recovery is 4-6 months. This requires a period of 4-6 weeks of non weight bearing on crutches and avoiding full knee flexion to protect the repaired tissue. It takes the meniscus 12 weeks to fully heal and so no running or jumping until after that time. Physical therapy begins right away to work on knee motion and strengthening to prepare the body for return to activity once the tissue has healed.
An interesting area of research more recently has been focusing on the use of biologic augmentation to meniscal repair surgery. This involves the use of either platelet rich plasma or bone marrow aspirate concentrate injected directly at the repair site to help promote tissue healing and collagen formation.

Dr. Mark Sando is an internationally recognized orthopaedic surgeon specializing in sports medicine, arthroscopy and injuries of the shoulder, knee and hip. He earned his medical degree from Case Western Reserve University School of Medicine and completed residency at the University of Maryland Medical Center and R Adams Cowley Shock Trauma Center. After residency, Dr. Sando went on to complete subspecialized training in Sports Medicine as a fellow at the prestigious Kerlan-Jobe Orthopaedic Clinic in Los Angeles, CA under the direction of Dr. Neal ElAttrache. He has worked with numerous college athletic programs and professional teams including the world champion Los Angeles Kings, Los Angeles Lakers, Los Angeles Dodgers, and Los Angeles Sparks. Dr. Sando has been with the Orthopaedic Medical Group of Tampa Bay since 2015. Full Bio